
Hypertensive Encephalopathy Presenting as Cadasil
Article Sidebar
Main Article Content
Abstract
Hypertensive encephalopathy is a less often clinical scenario of hypertensive emergency, typified by severe resistant hypertension and mental status changes. Besides that, Hypertensive encephalopathy is enkindled by meagre controlled primary or secondary cause of hypertension and is difficult to pin down the etiology, which can concretely affect the treatment outcome.
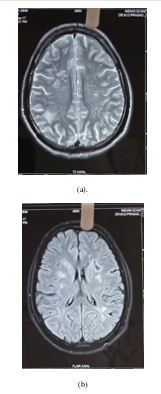
Furthermore we discuss regarding a young adult male who has a meagrely controlled hypertensive presenting with head ache, vomiting and behavioural changes. On examination patient had impaired recent memory with other systems being intact. Computed tomography showed diffuse cerebral edema and Magnetic resonance showed white matter hyper intensities on T2 weighted images involving subcortical white matter and temporal lobe with relative sparing of posterior lobes which is classical for CADASIL (cerebral autosomal dominant artery disease with leukoencephalopathy and subcortical infarcts). CADASIL is inherited as an autosomal dominant trait, results from a mutation on chromosome 19p13.12 involving the NOTCH 3 gene. Besides classical radiological features suggesting CADASIL, the clinical and single gene testing did not unveil the diagnosis. Despite sometimes having high blood pressure, the blood pressure dropped throughout the second week after admission. Taking the clinical improvement into consideration his diagnosis was changed to hypertensive encephalopathy. By varying clinical appearance and exhibiting seldom evident clinicoradiological separation, hypertensive encephalopathy sets itself apart. Understanding the clinical and radiological signs of hypertensive encephalopathy will aid in guiding therapy and preventing pointless and expensive studies.
Article Details
References
Zampaglione B, Pascale C, Marchisio M, et al.. Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension 1996;27:144–7. 10.1161/01.HYP.27.1.144 [PubMed] [CrossRef] [Google Scholar]
Karakis I, Macdonald JA, Stefanidou M, et al.. Clinical and radiological features of brainstem variant of hypertensive encephalopathy. J Vasc Interv Neurol 2009;2:172–6. [PMC free article] [PubMed] [Google Scholar]
Nagata M, Maeda M, Tsukahara H, et al.. Brain stem hypertensive encephalopathy evaluated by line scan diffusion-weighted imaging. Am J Neuroradiol 2004;25:803–6. [PMC free article] [PubMed] [Google Scholar]
Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol 2015;14:914–25. 10.1016/S1474-4422(15)00111-8 [PubMed] [CrossRef] [Google Scholar]
Hauser RA, Lacey DM, Knight MR. Hypertensive encephalopathy. magnetic resonance imaging demonstration of reversible cortical and white matter lesions. Arch Neurol 1988;45:1078–83. [PubMed] [Google Scholar]
Osman Y, Imam YZ, Salem K, et al.. Isolated Brainstem Involvement in a Patient with Hypertensive Encephalopathy. Case Rep Neurol Med 2013;2013:1–7. 10.1155/2013/540947 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
McKinney AM, Jagadeesan BD, Truwit CL. Central-variant posterior reversible encephalopathy syndrome: brainstem or basal ganglia involvement lacking cortical or subcortical cerebral edema. Am J Roentgenol 2013;201:631–8. 10.2214/AJR.12.9677 [PubMed] [CrossRef] [Google Scholar]
Gamanagatti S, Subramanian S. Hypertensive encephalopathy: isolated pons involvement mimicking central pontine myelinolysis. Korean J Radiol 2006;7:218–9. 10.3348/kjr.2006.7.3.218 [PMC free article] [PubMed] [CrossRef] [Google Scholar]